
And then there were three: A single-shot vaccine is the latest weapon to join the battle against COVID-19 in the United States.
On February 27, the U.S. Food and Drug Administration gave emergency use authorization for Johnson & Johnson’s vaccine against SARS-CoV-2, the coronavirus that causes COVID-19. South Africa is the only other country to OK Johnson & Johnson’s vaccine so far, though other countries are poised to follow suit.
The FDA determined that Johnson & Johnson’s vaccine meets the criteria for safety and effectiveness and that there is clear evidence that it may prevent COVID-19, the agency said in a statement.
“With today’s authorization, we are adding another vaccine in our medical toolbox to fight this virus,” said Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research.
Its authorization for emergency use in the United States – for people age 18 and older – follows similar authorizations in December for vaccines made by Moderna and by Pfizer and its German partner BioNTech.
Shortages of vaccines make the addition of a third safe and effective vaccine welcome. “We’re still in the midst of this deadly pandemic,” says Archana Chatterjee, Dean of the Chicago Medical School at Rosalind Franklin University of Medicine and Science.
“Authorization of this vaccine will help meet the needs at the moment,” she said February 26 after an FDA vaccine advisory committee unanimously voted to recommend Johnson & Johnson’s vaccine for emergency use.
But even as the pharmaceutical company readies to ship out 4 million doses, questions remain about how well the public will embrace the new shot.
On the one hand, people weary of struggling to set up not just one but two appointments to get the currently available double-dose vaccines may welcome one-stop shopping. And adding millions more vaccines to the pipeline should speed up efforts to get the vast majority of Americans protected.
But on the other hand, its efficacy results fall short of those reported for two shots of the mRNA vaccines made by Moderna (94.1 percent) and Pfizer (95 percent) (SN: 1/29/21; SN: 11/16/20; SN: 11/18/20). In real-world situations, a single shot of Pfizer’s vaccine was 74 percent to 85 percent effective at preventing hospitalizations (SN: 2/26/21).
In clinical trials, Johnson & Johnson’s vaccine was about 66 percent effective at preventing moderate and severe disease. Its efficacy rose to 85 percent when it came to preventing severe and critical cases requiring hospitalization.
Here’s what you need to know about the vaccine, which was developed by Johnson & Johnson’s subsidiary Janssen Pharmaceuticals:
How does it work?
Researchers engineered a common cold virus called adenovirus 26 to carry instructions for making the coronavirus’s spike protein into human cells. The human cells make the viral protein, which goads the immune system to make antibodies and train immune cells to attack the coronavirus, should the person encounter it later.
The engineered adenovirus 26, which has been altered so that it can’t cause disease, is the base for other vaccines made by Janssen, including an approved Ebola vaccine, and experimental vaccines against Zika, HIV and respiratory syncytial virus (RSV). Together, trials of those vaccines have tested the engineered virus in more than 193,000 people, including children, pregnant women and immunocompromised people. Those trials have shown that the technology has a good safety record.
Why is this one less effective than other authorized vaccines?
It may be unfair to directly compare the efficacy results. Johnson & Johnson’s vaccine was tested in the United States, South Africa, Brazil and other parts of Latin America when coronavirus variants that can escape some immune protection were circulating. Under the same conditions, the mRNA vaccines might be less effective, too.
This is also a single-shot vaccine. It’s efficacy is similar to that of a different two-dose adenovirus vaccine made by the University of Oxford and its partner AstraZeneca (SN: 11/23/20).
Johnson & Johnson has begun testing whether a second dose of its vaccine can boost efficacy. If a second dose improves efficacy, researchers worry that the new information could sow confusion among those who have already gotten the shot.
“If you bring out a single-dose vaccine … and later say that a second dose is clinically better enough that we recommend a second dose, you can see how that would be confusing,” Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, said during the FDA vaccine advisory board meeting.
Should I get the shot?
Yes, the experts say.
“We’re going to have to communicate effectively so people don’t feel they’re getting a second-rate product. It’s very good at what it does,” says Georges Benjamin, executive director of the American Public Health Association in Washington, D.C.
Although the Johnson & Johnson vaccine didn’t prevent moderate or severe illness as well as the mRNA vaccines do, “it’s going to protect, no matter what, for the part of the disease that we really care about, which is hospitalization, severe disease and death,” Benjamin says. “There’s no difference.”
As of February 25, more than 52,000 people were hospitalized in the United States fighting COVID-19, according to the COVID Tracking Project. That’s down from the record-setting daily peaks of more than 130,000 in early January and the lowest since early to mid-November. More than half a million people in the United States have now died from COVID-19.
In Johnson & Johnson’s clinical trial, two of the 19,514 people in the vaccine group were hospitalized with COVID-19 starting 14 days after vaccination. That compares with 29 hospitalizations among the 19,544 people in the placebo group. None of the vaccinated people died, but there were seven deaths related to COVID-19 in the placebo group. Those numbers are small and some researchers say the data aren’t clear-cut on the benefits.
“The data indicate that the vaccine is effective, but doesn’t prove that the vaccine is especially effective against moderate to severe COVID,” said Diana Zuckerman, president of the National Center for Health Research, a Washington, D.C.–based think tank that analyzes health research.
The data were also collected after only two months of follow-up. Normally, the FDA requires a year or more of data to fully approve a vaccine. Some questions about the vaccine can’t be answered with less than six months of data, Zuckerman said during a public comment period in the Feb. 26 advisory board hearing. “Let’s be very honest with the public about what we do know and what we won’t know” for some time to come.
For all the vaccines, no one knows how long immunity will last. And what’s already authorized might need to be tweaked if resistant variants become widespread. Booster shots may be needed, Benjamin says.
Most people probably won’t be able to choose which vaccine they get, but if the choice is taking the Johnson & Johnson vaccine or waiting months for an mRNA vaccine, “to me that’s not a close call. You should get the J&J now,” says Robert Wachter, who chairs the Department of Medicine at the University of California, San Francisco. “The best vaccine is the one you get today.”
How many people will be able to get the vaccine?
The company fell short of its goal to deliver 10 million doses by the end of February. But it can have 20 million doses by the end of March and 100 million by the end of June, a company official told a subcommittee of the U.S. House of Representatives Energy and Commerce Committee on February 23.
Because the vaccine is given as a single shot, each dose is enough to vaccinate a person. Pfizer’s and Moderna’s vaccines require two shots for complete efficacy.
“The fact that it’s a single dose lends itself to be a game changer,” says Krishna Udayakumar, director of the Duke Global Health Institute in Durham, N.C.
People who have a fear of needles, or those who can’t take time off work or don’t have transportation to vaccination sites might prefer a single shot over the two-dose mRNA vaccines.
“We have poorly housed people who come to the ER,” Wachter says. “They don’t have a doctor. They don’t have a house and we’re going to try to vaccinate them and bring them back in a month? It’s just not going to work.” A single-dose vaccine would be ideal in that setting.
Plus, the vaccine doesn’t require freezing. It can be stored in a standard refrigerator for up to three months. That makes it easier to use in places that don’t have easy access to freezers needed to keep the mRNA vaccines fresh.
With the three authorized vaccines, the United States may have enough doses by the end of the summer to vaccinate everyone, Udayakumar says.
The quicker the United States can vaccinate vulnerable populations, the sooner it might begin sharing vaccines with low-income countries through the World Health Organization’s COVAX program (SN: 2/26/20).
“We still have 130 countries that have had zero vaccinations,” says Udayakumar. “In the U.S., we’ve purchased more vaccine than we could ever use.”
 A new treatment could restore some mobility in people paralyzed by strokes
A new treatment could restore some mobility in people paralyzed by strokes 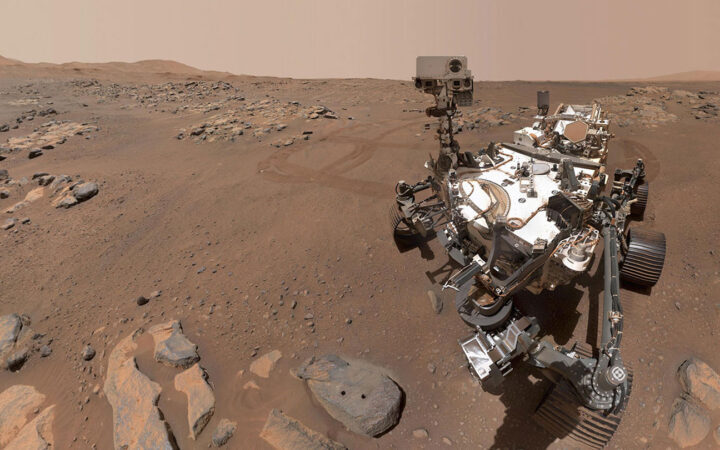 What has Perseverance found in two years on Mars?
What has Perseverance found in two years on Mars? 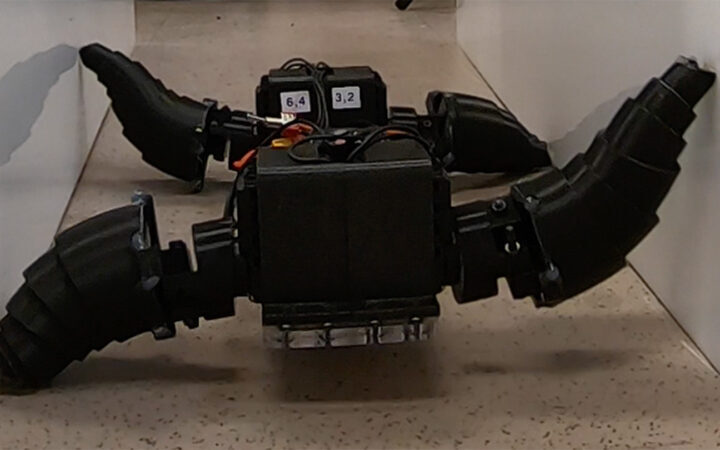 This robot automatically tucks its limbs to squeeze through spaces
This robot automatically tucks its limbs to squeeze through spaces  Greta Thunberg’s new book urges the world to take climate action now
Greta Thunberg’s new book urges the world to take climate action now  Glassy eyes may help young crustaceans hide from predators in plain sight
Glassy eyes may help young crustaceans hide from predators in plain sight  A chemical imbalance doesn’t explain depression. So what does?
A chemical imbalance doesn’t explain depression. So what does?